David Walter Banks/The Washington Post/Getty Images
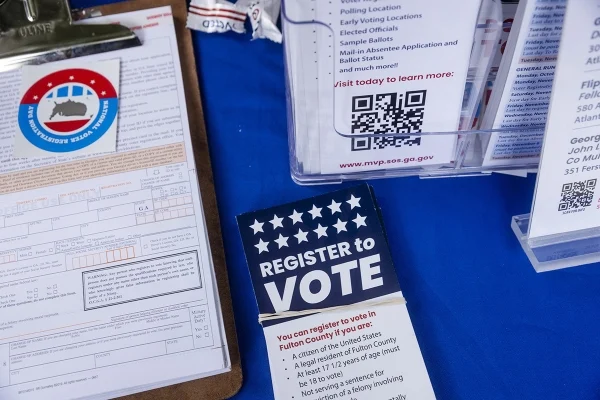
Ahead of the 2026 primaries, the North Carolina State Board of Elections rejected a plan Tuesday to open an early-voting center on the Greensboro campus of North Carolina A&T State University, according to NC Newsline.
The Republican-controlled board also voted to close the existing early-voting centers at Elon University and Western Carolina University.
After the vote, a group of N.C. A&T students who traveled to Raleigh for the board meeting gathered in the boardroom, protesting the decision. But Francis De Luca, chair of the board, threatened to call the cops if they didn’t leave, according to the news outlet.
De Luca, who voted against the early-voting sites, said he’s not in favor of them for numerous reasons. “There’s no parking,” he said. “They may set aside parking; if it’s filled, you’re going to get a ticket. We don’t put sites where there’s no parking anywhere else.”
But Siobhan Millen, a Democratic member of the board who voted for the voting centers, said the move puts “student voting is in the crosshairs.”
Without voting sites on campus, students—including many who don’t own cars—will have to travel to off-campus precincts, though some in favor of axing campus polling centers have described them as redundant. Zayveon Davis, a voter engagement leader at N.C. A&T, said the HBCU would provide shuttles to take students to the nearest polling place.
Nonetheless, he called the decision “disappointing” and reflective of broader Republican-led efforts to restrict voting access, especially for marginalized communities.
“I hope that everybody leaves here knowing that your voice does matter. Your vote does matter,” he told NC Newsline. “And if it didn’t, they wouldn’t be working this hard to take it away.”
A total of 14 centers and institutes will be decommissioned, according to a budget reductions presentation to the board in November.
Tar_Heel_Rob/iStock/Getty Images
The University of North Carolina at Chapel Hill will close its area studies centers in 2026, faculty members within the centers told Inside Higher Ed.
The six centers—the Center for European Studies, the African Studies Center, the Carolina Asia Center, the Center for Middle East and Islamic Studies, the Institute for the Study of the Americas and the Center for Slavic, Eurasian and East European Studies—are all expected to close at some point next year.
“Our leadership team is taking a thoughtful and targeted approach, looking into areas that can be streamlined for greater efficiency, strengthening our operations while meeting our fiduciary responsibility to the people of North Carolina,” the UNC media relations department said in a statement. “A number of factors were taken into consideration while evaluating Centers and Institutes and some programs have been identified to be sunset [sic] in 2026. The list is not finalized at this time.”
Further updates will come after the January Board of Trustees meeting, the spokespeople said.
In a “budget reductions update” to the board’s finance and infrastructure committee in November, university officials said they planned to save $7 million in annual spending from “centers and institute reductions” made over several years, with a goal of $3 million in budget reductions before the end of this fiscal year in June 2026. A total of 14 centers and institutes will be decommissioned, according to the presentation.
This story about children with disabilities was produced by The Hechinger Report, a nonprofit, independent news organization focused on inequality and innovation in education. Sign up for the Hechinger newsletter.
COLUMBUS, Ohio — When Selina Likely became director of the Edwards Creative Learning Center six years ago, she knew there was one longstanding practice that she wanted to change. For as long as she had taught at the thriving child care center, it had turned away many children with disabilities such as autism and Down syndrome. The practice was even encoded in the center’s handbook as policy.
Likely, the parent of a child with a disability, wanted to stop telling families no, but she knew that to do that she and her staff would need more support. “I said, ‘Let’s start getting training and see what we can do.’”
Not too long after, her effort received a big boost from a state-funded initiative in Ohio to strengthen child care teachers’ knowledge and confidence in working with young kids with disabilities and developmental delays. That program, Ohio PROMISE, offers free online training for child care workers in everything from the benefits of kids of all abilities learning and playing together to the kinds of classroom materials most helpful to have on hand. It also offers as-needed mentorship and support from trained coaches across the state.
Related: Young children have unique needs, and providing the right care can be a challenge. Our free early childhood education newsletter tracks the issues.
Child care providers across the country — including large, established centers and tiny home-based programs — struggle to meet the needs of children with disabilities, according to a 2024 report from the U.S. Government Accountability Office. More than a quarter of parents of children with disabilities said they had a lot of difficulty finding appropriate care for their kids. And even those who do find a spot regularly encounter challenges, like having their children excluded from extracurricular activities such as field trips and even academic instruction.
“It’s really hard to find child care for this population, we heard that loud and clear,” said Elizabeth Curda, a director on the GAO’s Education, Workforce and Income Security team and a coauthor of the report. Even the most well-resourced centers report that they struggle to meet the needs of children with disabilities, according to Curda.
There’s a lot of desire at the grassroots level to change that. Ohio PROMISE and a few other recent initiatives provide models for how to expand the capacity — and the will — of child care centers to serve the more than 2 million U.S. children age 5 or below who have a disability or developmental delay.
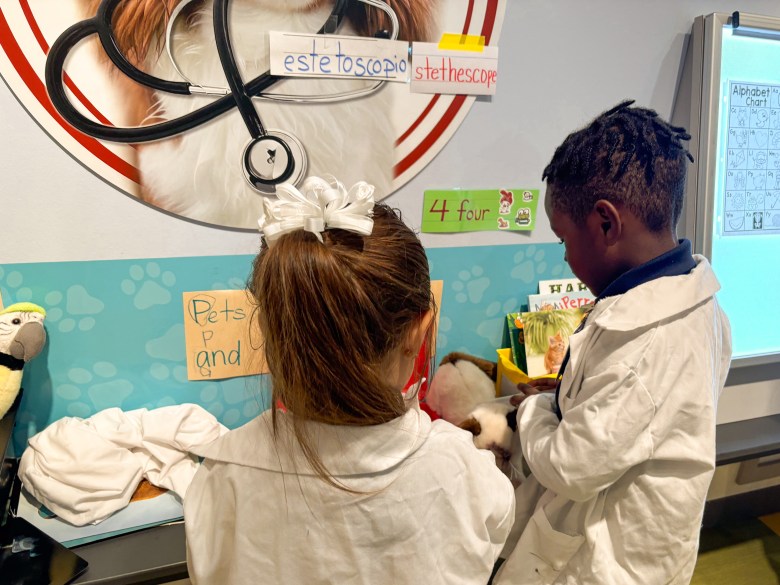
Cards on the walls at Edwards Creative Learning Center display the signs for different letters so students — whether nonverbal or not — can all learn sign language. Credit: Sarah Carr/The Hechinger Report
In Vermont, for instance, officials hope to soon unveil a free, on-demand training program aimed at helping child care teachers have more inclusive classrooms. And officials in Ohio’s Summit County, home to Akron, report growing interest from other counties in creating programs based on Summit’s more than decade-old model that provides in-person training for child care operators in inclusion of children with disabilities.
“We’re helping to create child care centers that feel they can handle whatever comes their way, especially when it comes to significant behavior concerns,” said Yolanda Mahoney, the early childhood center support supervisor for Summit County’s disabilities board.
The federal government until recently encouraged the creation of such models. In 2023, the federal Department of Education and Department of Health and Human Services issued a joint statement urging states to take steps to support inclusion in early childhood settings, including strengthening training and accountability.
Under the current president, federal momentum on the issue has largely stalled. While the administration of President Donald Trump hasn’t directly attacked inclusion in the context of special education, the president has criticized the term more broadly — especially when it comes to diversity, equity and inclusion. That can create uncertainty and a chilling effect on advocates of inclusion efforts of all kinds.
Funding for some inclusion efforts is also in jeopardy. States rely on Medicaid, which faces nearly $1 trillion in cuts over the next decade, to pay for early intervention programs for children birth to age 3 with developmental delays and disabilities. Trump has also proposed eliminating Preschool Development Grants, which states such as Vermont and Illinois have used to expand support of young children with disabilities.
That means over the next few years, progress on inclusion in child care settings could hinge largely on state and local investment. It helps that there’s a “real desire” among providers to enroll more children with disabilities, said Kristen Jones, an assistant director on the GAO’s education, workforce and income security team, who also worked on the report. “But there’s also a concern that currently they can’t do that in a safe way” because of a lack of training and resources.
In Ohio, the idea for Ohio PROMISE came after an appeal in 2022 from Republican Gov. Mike DeWine. He reported that families were coming to him saying they couldn’t find child care for their kids with disabilities.
“He said, ‘Come to me with ideas to solve that problem,’” recalled Wendy Grove, a senior adviser in the Ohio Department of Children and Youth who spearheaded development of the program.
Grove and her colleagues had already been working on a related effort. In 2020, Ohio won a federal grant that included help exploring how well — or not — children with disabilities were being included in child care and early education settings. DeWine liked the idea Grove’s team presented of morphing that work into a state-led effort to strengthen training and support for child care teachers. They also proposed more direct support to families, including the extension of child care vouchers to families with incomes above the poverty level, with a higher reimbursement rate for children with disabilities.
The training, which debuted about two years ago, is provided in three levels. Jada Cutchall, a preschool teacher at Imaginative Beginnings, an early learning center just outside of Toledo, recently completed the third tier, which for her included customized coaching. Cutchall’s coach helped her create communication tools for a largely nonverbal student, she said, including a board with pictures children can point to if, for example, they want to go to the bathroom or try a different playground activity.
As a result, Cutchall said, she has watched kids with disabilities, including those with speech impairments and autism, engage much more directly with their classmates. “They have the courage to ask their peers to play with them — or at least not distance themselves as much as they usually would,” she said. All of the children in the classroom have benefited, she added, noting that kids without disabilities have taken an interest in learning sign language, strengthening their own communication skills and fostering empathy.
Child care programs where one teacher and one administrator have completed some of the training earn a special designation from the state, which may eventually be tied to the opportunity to get extra funding to serve children with disabilities. In Ohio PROMISE’s first year, 1,001 child care centers — about 10 percent of the total number in Ohio — earned that designation, according to Grove.
For the last six years, Selina Likely has overseen the Edwards Creative Learning Center, where she’s steadily tried to enroll more children with disabilities and developmental delays. Credit: Sarah Carr/The Hechinger Report
The effort costs a little over $1 million in state dollars each year, with most of that paying for several regional support personnel who work directly with centers as mentors and advisers. Over the last two years, Ohio has seen a 38 percent increase in the number of children in publicly funded centers who qualify for the higher voucher reimbursement rate for children with disabilities, which can be double the size of the standard voucher.
Grove hopes that ultimately the effort plays a role in narrowing a critical and stubborn gap in the state: about 27 percent of children without disabilities show readiness on state standards for kindergarten; only 14 percent of children with disabilities do. Since so few disabilities exhibited at that age are related to intellectual or cognitive functioning, “we shouldn’t see that gap,” said Grove. “There’s no real reason.”
One goal of the new efforts is to reduce the number of young children with disabilities who are expelled from or pushed out of care. Those children are frequently asked to leave for behaviors related to their disability, the GAO report found.
Several years ago, a child care center in Columbus expelled Meagan Severance’s 18-month-old son for biting a staff member. The boy has several special needs, including some related to attention deficit hyperactivity disorder. Severance brought him to Edwards Creative Learning Center, where not too long after Selina Likely shifted into the role of director. The boy also bit a staff member there — not uncommon behavior for toddlers, especially those with sensory sensitivities and communication challenges.
Likely was determined to work with the child, not expel him. “They put in time and effort,” said Severance. “The response wasn’t, ‘He bit someone, he’s gone.’”
Likely empathized. Decades earlier, her own daughter had been expelled from a child care center in her hometown of Mansfield, Ohio, for biting.
“I was so angry and mad at the time — how are you going to kick out a 1-year-old?” she said. The center director didn’t think at all about how to help her child, Likely recalled, instead asking Likely what might be happening at home to make the child want to bite. She said she got no notice or grace period to find a new placement. “That left me in a disheartened place,” she said. “I was like, ‘I still have to go to work.”
Seventeen years old at the time, she was inspired by the injustice of the situation to quit her job in a factory and apply to be an assistant in a child care program. She’s been in the industry ever since, gradually trying to make more space for children like her daughter, who was later diagnosed with autism.
Meagan Severance, a parent and teacher at the Edwards center, has worked in recent years to make her classroom more inclusive for children with all different abilities. Credit: Sarah Carr/The Hechinger Report
As director, Likely displays the nameplate “chaos coordinator” on her desk. And she’s taken the stance that the center should at least try to work with every kid. She and some of her teachers have completed the first two tiers of the Ohio PROMISE training, as well as some related sessions available from the state. Likely estimates that about 10 percent of the children in her center have a diagnosed disability or developmental delay.
Liasun Meadows, whose son has Down syndrome, chose Edwards several years ago for her then 1-year-old over another program better known for its work with children with disabilities. She has not been disappointed.
Parents of kids with disabilities watch their children like a hawk, she said. “There are certain things you notice that you don’t expect others to notice, but they do at Edwards. They’ve been growing and learning alongside him.”
Severance, whose son is now 8, works at the center these days, leading the 3-year-old room, which includes two children who are largely nonverbal. She’s made the classroom more inclusive, adding fidget toys for children with sensory issues, rearranging the classroom to create calming areas, providing communication books to nonverbal children so they can more easily express needs and wants, and teaching everyone some sign language.
“For a while there was segregation in the classroom” between the kids with disabilities and those without, Severance said. But that’s lessened with the changes. “Inclusion has been good for the kids who are verbal — and nonverbal,” she said.
As in Ohio, state officials in Vermont turned to online training to help ensure young children with disabilities aren’t denied quality care. The state should soon debut the first parts of a new training program, focusing on outreach to child care administrators and support for neurodivergent children. The state wanted to focus on center leaders first because “directors that are comfortable with inclusion lead programs that are comfortable with inclusion,” said Dawn Rouse, the director of statewide systems in Vermont’s Child Development Division.
One tool for supporting and calming children with sensory issues is keeping a healthy supply of fidget toys and Pop-Its on hand. Credit: Sarah Carr/The Hechinger Report
Vermont also pumped millions of dollars into a separate program, known as the Special Accommodations Grant, that supports young children with disabilities. Since 2009 the state has set aside $300,000 a year that child care centers can tap to provide services for individual children with disabilities. It might help buy specialized equipment for a child with cerebral palsy, for instance, or be used to hire a full- or part-time aide.
The $300,000 has been maxed out every year, Rouse said. And after the pandemic, the need — and the number of applications — surged.
As a result, the state allocated some federal American Rescue Plan and Preschool Development Grant dollars to increase spending on the program by about sevenfold — to between $2 million and $2.5 million annually — an amount Rouse still describes as a “Band-Aid.” Without access to the grants, “we see a lot of children being asked to leave programs,” Rouse said. “That’s not good for any child, but for children with specialized developmental needs it’s particularly bad.”
Over time, Likely hopes, her Ohio center can play a small role in reducing that instability, although the center hasn’t yet been able to work with all such children it wants to. Likely recalls one toddler with a severe disability who climbed up anything he could. There wasn’t enough money to pay for what the child really needed: a full-time aide. “It’s hard when you know you’ve tried but still have to say no,” she said. “That breaks my heart more than anything.”
On one June morning, the center’s teachers acknowledged and celebrated several milestones in its work on inclusion, big and small. One child in the 3-year-old classroom with fine and gross motor challenges was drinking independently from a bottle. The preschool classroom held its first graduation ceremony, translated partly into sign language. All of the kids, no matter their challenges, were set to go on field trips to Dairy Queen and the zoo.
Likely dreams of someday running a center where about half of the children have a disability or delay. It may be years off, she said, but as with the milestones she sees scores of children at the center reach every day, “There’s a way — if there’s a will.”
Sarah Carr is a fellow at New America, focused on reporting on early childhood issues.
The Hechinger Report provides in-depth, fact-based, unbiased reporting on education that is free to all readers. But that doesn’t mean it’s free to produce. Our work keeps educators and the public informed about pressing issues at schools and on campuses throughout the country. We tell the whole story, even when the details are inconvenient. Help us keep doing that.
(Image: Mass General is Harvard University Medical School’s teaching hospital.)
For decades, America’s elite university medical centers have been the epitome of healthcare research and innovation, providing world-class treatment, education, and cutting-edge medical advancements. Yet, beneath this polished surface lies a troubling legacy of medical exploitation, systemic inequality, and profound injustice—one that disproportionately impacts marginalized communities. While the focus has often been on racial disparities, this issue is not solely about race; it is also deeply entangled with class. In recent years, books like Medical Apartheid by Harriet Washington have illuminated the history of medical abuse, but they also serve as a reminder that inequality in healthcare goes far beyond race and touches upon the economic and social circumstances of individuals.
The term Medical Apartheid, as coined by Harriet Washington, refers to the systemic and institutionalized exploitation of Black Americans in medical research and healthcare. Washington’s work examines the history of Black Americans as both victims of medical experimentation and subjects of discriminatory practices that have left deep scars within the healthcare system. Yet, the complex interplay between race and class means that many poor or economically disadvantaged individuals, regardless of race, have also faced neglect and exploitation within these prestigious medical institutions. The legacy of inequality within elite university medical centers, therefore, is not limited to race but is also an issue of class disparity, where wealthier individuals are more likely to receive proper care and access to cutting-edge treatments while the poor are relegated to substandard care.
Historical examples of exploitation and abuse in medical centers are well-documented in Washington’s work, and contemporary lawsuits and investigations reveal that these systemic problems still persist. Poor patients, especially those from marginalized racial backgrounds, are often viewed as expendable research subjects. The lawsuit underscores the intersectionality of race and class, arguing that these patients’ socio-economic status exacerbates their vulnerability to medical exploitation, making it easier for institutions to treat them as less than human, especially when they lack the resources or power to contest medical practices.
One of the most critical components of this issue is the stark contrast in healthcare access between the wealthy and the poor. While elite university medical centers boast state-of-the-art facilities, cutting-edge treatments, and renowned researchers, these resources are often not equally accessible to all. Wealthier patients are more likely to have the financial means to receive the best care, not just because of their ability to pay but because they are more likely to be referred to these prestigious centers. Conversely, low-income patients, especially those without insurance or with inadequate insurance, are often forced into overcrowded public hospitals or community clinics that are underfunded, understaffed, and unable to provide the level of care available at elite institutions.
The issue of class inequality within medical care is evident in several key areas. For instance, studies have shown that low-income patients, regardless of race, are less likely to receive timely and appropriate medical care. A 2019 report from the National Academy of Medicine found that low-income patients are often dismissed by healthcare professionals who underestimate the severity of their symptoms or assume they are less knowledgeable about their own health. In addition, patients from lower socio-economic backgrounds are more likely to experience medical debt, which can lead to long-term financial struggles and prevent them from seeking care in the future.
Moreover, class plays a significant role in the underrepresentation of poor individuals in medical research, which is often conducted at elite university medical centers. Historically, clinical trials have excluded low-income participants, leaving them without access to potentially life-saving treatments or advancements. Wealthier individuals, on the other hand, are more likely to be invited to participate in research studies, ensuring they benefit from the very innovations and breakthroughs that these institutions claim to provide.
Class-based disparities are also reflected in the inequities in medical professions. The road to becoming a physician or researcher in these elite institutions is often paved with significant economic barriers. Medical students from low-income backgrounds face steep financial challenges, which can hinder their ability to gain acceptance into prestigious medical schools or pursue advanced research opportunities. Even when low-income students do manage to enter these programs, they often face biases and discrimination in clinical settings, where their abilities are unfairly questioned, and their economic status may prevent them from fully participating in research or other educational opportunities.
Yet, the inequities within these institutions don’t stop at the patients. Behind the scenes, workers at elite university medical centers, particularly those from working-class and marginalized backgrounds, face their own form of exploitation. These medical centers are not only spaces of high medical achievement but also sites of labor stratification, where workers in lower-paying roles are largely people of color and often immigrants. Support staff—such as janitors, food service workers, custodians, and administrative assistants—are often invisible but essential to the functioning of these hospitals and research institutions. These workers face long hours, poor working conditions, and low wages, all while contributing to the daily operations of elite medical centers. Many of these workers, employed through third-party contractors, lack benefits, job security, or protections, leaving them vulnerable to exploitation.
Custodial workers, who are often exposed to hazardous chemicals and physically demanding work, may struggle to make ends meet, despite playing a crucial role in maintaining the hospital environment. Similarly, food service workers—many of whom are Black, Latinx, or immigrant—also work in demanding conditions for low wages. These workers frequently face job insecurity and are not given the same recognition or compensation as the high-ranking physicians, researchers, or administrators in these centers.
At the same time, the stratification in these institutions extends beyond support staff. Medical researchers, residents, and postdoctoral fellows—often young, early-career individuals, many from working-class backgrounds or communities of color—are similarly subjected to precarious working conditions. These individuals perform much of the vital research that drives innovation at these centers, yet they often face exploitative working hours, low pay, and job insecurity. They are the backbone of the institution’s research output but frequently face barriers to advancement and recognition.
The higher ranks of these institutions—senior doctors, professors, and researchers—enjoy financial rewards, job security, and prestige, while those at the lower rungs continue to experience instability and exploitation. This division, which mirrors the economic and racial hierarchies of broader society, reinforces the very class-based inequalities these medical centers are meant to address.
In recent years, some progress has been made in addressing these inequalities. Many elite universities have implemented diversity and inclusion programs aimed at increasing access for underrepresented minority and low-income students in medical schools. Some institutions have also begun to emphasize the importance of cultural competence in training medical professionals, acknowledging the need to recognize and understand both racial and economic disparities in healthcare.
However, critics argue that these efforts, while important, are often superficial and fail to address the root causes of inequality. The institutional focus on “diversity” and “inclusion” often overlooks the more significant structural issues, such as the affordability of education, the class-based access to healthcare, and the economic barriers that continue to undermine the ability of disadvantaged individuals to receive quality care.
In addition to acknowledging racial inequality, it is crucial to tackle the broader issue of class within the healthcare system. The disproportionate number of Black and low-income individuals suffering from poor healthcare outcomes is a direct result of a system that privileges wealth and status over human dignity. To begin addressing these issues, we need to move beyond token diversity initiatives and work toward policy reforms that focus on economic access, insurance coverage, and the equitable distribution of medical resources.
Scholars like Harriet Washington, whose work documents the intersection of race, class, and healthcare inequality, continue to play a pivotal role in bringing attention to these systemic injustices. Washington’s book Medical Apartheid serves as a historical record but also as a call to action for creating a healthcare system that genuinely serves all people, regardless of race or socio-economic status. The fight for healthcare equity must, therefore, be a dual one—against both racial and class-based disparities that have long plagued our medical institutions.
The story of Henrietta Lacks, as told in The Immortal Life of Henrietta Lacks by Rebecca Skloot, exemplifies the longstanding exploitation of marginalized individuals in elite university medical centers. The case of Lacks, whose cells were taken without consent by researchers at Johns Hopkins University, brings to light both the historical abuse of Black bodies and the profit-driven nature of academic medical research. Johns Hopkins, one of the most prestigious medical centers in the world, has been complicit in the kind of exploitation and neglect that these institutions are often criticized for—issues that disproportionately affect not only Black Americans but also economically disadvantaged individuals.
The Black Panther Party’s healthcare activism, as chronicled by Alondra Nelson in Body and Soul, also directly challenges elite medical institutions’ failure to provide adequate care for Black and low-income communities. Nelson’s work reflects how, even today, these institutions are often slow to address the systemic issues of health disparities that activists like the Panthers fought against.
Recent lawsuits against elite medical centers further underscore the importance of holding these institutions accountable for their role in perpetuating medical exploitation and inequality. In An American Sickness by Elisabeth Rosenthal, the commercialization of healthcare is explored, highlighting how university hospitals and medical centers often prioritize profits over patient care, leaving low-income and marginalized groups with limited access to treatment. Rosenthal’s work highlights the role these institutions play in a larger system that disproportionately benefits wealthier patients while neglecting the most vulnerable.
A Global Comparison: Countries with Better Health Outcomes
While the United States struggles with systemic healthcare disparities, other nations have shown that equitable healthcare outcomes are possible when class and race are not barriers to care. Nations with universal healthcare systems, such as those in Canada, the United Kingdom, and many Scandinavian countries, consistently rank higher in overall health outcomes compared to the U.S.
For instance, Canada’s single-payer system ensures that all citizens have access to healthcare, regardless of their income. This system reduces the financial burdens that often lead to delays in care or avoidance of treatment due to costs. According to the World Health Organization, Canada has better health outcomes on a variety of metrics, including life expectancy and infant mortality, compared to the U.S., where medical costs often lead to unequal access to care.
Similarly, the United Kingdom’s National Health Service (NHS) provides healthcare free at the point of use for all citizens. Despite challenges such as funding constraints and wait times, the NHS has been successful in ensuring that healthcare is a right, not a privilege. The U.K. consistently ranks higher than the U.S. in terms of access to care, health outcomes, and overall public health.
Nordic countries, such as Norway and Sweden, also exemplify how universal healthcare can lead to better outcomes. These countries invest heavily in public health and preventative care, ensuring that even their most marginalized citizens receive the necessary medical services. The result is a population with some of the highest life expectancies and lowest rates of chronic diseases in the world.
These nations show that, while access to healthcare is a critical issue in the U.S., the challenge is not a lack of innovation or capability. Instead, it is the systemic barriers—both racial and economic—that persist in elite medical centers, undermining the potential for universal health equity. The U.S. could learn from these nations by adopting policies that reduce economic inequality in healthcare access and focusing on preventative care and public health strategies that serve all people equally.
Ultimately, the dark legacy of elite university medical centers is not something that can be erased, but it is something that must be acknowledged. Only by confronting this painful history, alongside addressing class-based disparities, can we begin to build a more just and equitable healthcare system—one that serves everyone, regardless of race, background, or socio-economic status. Until this happens, the distrust and skepticism that many marginalized communities feel toward these institutions will continue to shape the landscape of American healthcare. The path forward requires a concerted effort to address both racial and class-based inequities that have defined these institutions for far too long. The U.S. can, and must, strive for healthcare outcomes akin to those seen in nations that have built systems prioritizing equity and fairness—systems that put human dignity over profit.
For decades, work-life balance has been seen as the gold standard of career success. The idea suggests that professionals should allocate time and energy evenly between work and personal life, ensuring equilibrium between competing responsibilities. But in reality, balance is often an illusion—an unattainable tightrope walk that leaves individuals feeling guilty, unfulfilled and stretched too thin.
The workforce of today—and especially the workforce of tomorrow—no longer aspires to a segmented life. Instead, workers seek career and life integration, a holistic approach where career, personal growth and well-being are deeply interconnected. Unlike the concept of work-life balance, which implies a constant trade-off, career and life integration builds synergy between personal and professional aspirations.
Workday’s Global Workforce Report found that employees who perceive their work as meaningful feel 37 percent more accomplished than those who don’t, even when facing workloads they describe as “challenging.” An Inside Higher Ed Career Advice piece written by a University of Michigan administrator explored the importance of integrating values into the career exploration process. Additionally, research highlighted in the Journal of Personalityindicates that young adults’ personal values significantly influence their career-related preferences, suggesting a strong desire for roles that reflect their core values.
If higher ed institutions continue to treat career development as separate from personal well-being, they will fail to meet the evolving needs of students and professionals alike. Career centers must evolve into career and life design labs—hubs of lifelong guidance, personal development and future readiness. This piece outlines five strategic imperatives that institutions must embrace to lead this transformation.
Moving from work-life balance to career and life integration.
The traditional work-life balance model assumes a strict separation between career and personal life, often emphasizing boundaries rather than synergy. The statistics tell a compelling story:
A Deloitte study found that 66 percent of employees report feeling chronically overworked or burned out despite efforts to maintain work-life balance.
Research from Gallup indicates that 76 percent of millennials believe a successful career should seamlessly integrate with personal fulfillment rather than be kept separate.
A recent Moodle study indicates that job burnout has reached an all-time high of 66 percent in 2025.
Campus career services leaders must reframe their approach. Students need tools to design careers that complement their life aspirations rather than forcing them to choose between professional success and personal fulfillment.
Most students and alumni struggle with clarity—they pursue careers based on external pressures rather than intrinsic motivations. Career centers must facilitate career and life vision workshops to help individuals align their inner purpose with external opportunities. By integrating career and life design principles into career services, institutions empower students to prototype different pathways, develop adaptability and connect their academic and professional lives with personal meaning.
By using a reflective, experiential approach, students learn that career development is not a rigid ladder but a fluid, evolving process.
Integrating emotional agility into career coaching.
One of the greatest barriers to success is not external—it’s internal. It is not a lack of skills. It is a lack of confidence, clarity and emotional agility. Many students enter the workforce grappling with impostor syndrome, career anxiety and fear of failure. A research study titled “The Impostor Phenomenon,” published in the International Journal of Behavioral Science, shows that over 70 percent of people experience impostor syndrome at some point in their lives.
Institutions must integrate emotional intelligence training into their strategic plans. Students need to learn how to navigate career uncertainty with resilience rather than fear. Instead of merely offering job search strategies, career coaches should incorporate cognitive reframing techniques to help students shift from self-doubt to empowerment. This involves helping students recognize negative thought patterns and replace them with action-oriented mindsets.
For instance, instead of viewing rejection as a failure, students should be encouraged to see it as an iteration in the career and life design process. Career setbacks, industry changes and professional pivots are inevitable.
Practical steps for career centers:
Train career coaches in cognitive-behavioral coaching techniques to help students recognize and reframe self-limiting narratives.
Integrate self-awareness exercises that help students identify core fears (of failure, rejection or inadequacy) and develop action plans to overcome them with emotional strength.
Provide group coaching sessions focused on overcoming impostor syndrome, building confidence and developing a growth mindset.
Use AI-driven career reflection tools to help students track their confidence growth over time.
Incorporate mindfulness practices and journaling into safe spaces and welcoming career and life design studios to help students reframe failure as part of their evolving unique narrative.
Emotional agility is a core component of career development. Success today isn’t about having the perfect career path—it’s about navigating uncertainty with emotional agility. Career services must equip students with resilience and adaptability to thrive in ever-changing industries.
Merging personal, career and professional development.
Career and life design should be deeply personal, shaped by self-awareness, curiosity and personal reflection. We mention “personal” first, because we begin with the person.
Career services has historically focused on résumé reviews, job placement and networking strategies—important elements, but not enough for long-term success. A 2023 report by the National Association of Colleges and Employers found that students who integrate personal development with career planning—through leadership training, mentorship and values-based exploration—are significantly more career-ready upon graduation. Rather than pushing students toward the highest-paying or most prestigious jobs, career centers should help them define success on their own terms.
Practical steps for career centers:
Develop integrated mentorship networks that connect students with professionals who exemplify career and life integration.
Help students build personalized business plans that help them take ownership of the story they are both writing and telling.
Leverage design thinking principles, encouraging students to experiment with career pathways that embrace uncertainty, adaptability and iterative learning rather than rigid, predetermined plans.
AI can assist in career trajectory mapping, skills assessment and predictive job market insights, while human coaches focus on deep coaching, the power of stories and career and life integration strategies.
Considering AI-powered hyperpersonalized career coaching.
While traditional career advising has relied heavily on in-person interactions, the next evolution of career services will be AI-empowered, data-informed and hyperpersonalized. AI-driven career exploration tools can analyze a student’s experiences to offer real-time, customized career insights. AI agents such as the 24-7 virtual Career and Life Design Lab provide personalized career simulations, self-actualization exercises and self-realization insights to help individuals align their career paths with their purpose.
This mindset shift in career services will blend AI and human coaching. AI can assist in career trajectory mapping, skills assessment and predictive job market insights, while human coaches focus on deep coaching, the power of stories and career and life integration strategies. This synergy allows for scalable yet deeply personalized career services.
Practical steps for career centers:
Integrate AI-driven solutions and experiential learning methodologies.
Introduce future-self mapping, where students interview their future selves and map out short- and long-term goals.
Use reverse-engineering techniques, working backward from the desired impact to identify the necessary skills, experiences and trajectories.
Implement AI-powered career simulations, allowing students to test and refine career decisions in a risk-free environment that tackles limiting beliefs and impostor syndrome.
Scaling lifelong learning beyond graduation.
The future of work demands continuous upskilling, reskilling and career agility. Institutions must create a culture of lifelong learning, where students and alumni receive ongoing support throughout their careers. Career services must expand their scope to lifelong learning and helping students and alumni develop not résumés, but portfolios of experiences.
Practical steps for career centers:
Create career and life integration circles, where alumni engage in peer coaching, mentorship and accountability partnerships.
Offer subscription-based career services, ensuring alumni have access to coaching, upskilling and career reinvention programs throughout their professional lives.
Establish annual career and life re-evaluation workshops, helping alumni recalibrate their career and life vision.
Conclusion: The New Paradigm
The future of work is not about balance. It is about integration. By embedding the career and life design theoretical framework into institutional frameworks, universities can better equip students for a rapidly changing world. Colleges and universities that fail to adapt will be left behind, while those that embrace career and life design—leveraging both AI and a holistic approach to personal, career and professional development—will supercharge their teams with scale and empower students to craft lives of purpose, adaptability and lasting impact.
The question is no longer whether career centers should evolve—it is whether they can afford not to.
Does your career center offer group coaching sessions focused on confidence building, growth mindset or related topics? Tell us about it.
HOUSTON — Jefferson Early Learning Center bears little resemblance to elementary schools many adults recall attending in their earliest years. The classrooms have child-sized boats and construction vehicles children can play on, and ceilings painted to resemble outer space. There are no desks — all space is devoted to learning through play. Windows are low to the ground so children can easily look outside. The gym floor is made of “pre-K friendly” layered vinyl, rather than hardwood, to cushion inevitable trips and falls. Hallways are lined with a corrugated plastic for wiggly fingers to touch as children transition to other locations.
Children love coming to the building, said teacher Cathy Delamore. “They feel like they own it.”
Alief Independent School District, which serves about 40,000 children in west Houston, is one of a growing number of districts across the country to pump money into creating a building that is tailor-made for pre-kindergarteners. Its new facility cost about $21 million and enrolls nearly 400 4- and 5-year-olds. By making the investment, school leaders are trying to avoid some of the pitfalls of placing young children in buildings designed for older students, including lost learning time when tiny feet have to meander down long hallways to bathrooms and cafeterias. Research suggests that when designed well, buildings can contribute to better outcomes for children. Creators of the Reggio Emilia approach to early learning, an educational philosophy that emphasizes child-led learning, even refer to the environment as the “third teacher” in a classroom.
A Gulf Coast themed classroom at Jefferson Early Learning Center. The themed classrooms reflect local careers and locations to help children connect what they learn with their local environment. Credit: Jackie Mader/The Hechinger ReportThe “Space City” classroom at Jefferson Early Learning Center is an homage to the local NASA space center. Credit: Jackie Mader/The Hechinger Report
Over the past few years, educators have grown aware of the benefits of a personalized pre-K environment, said Melissa Turnbaugh, a senior principal at the architecture firm PBK, which has designed more than 240 elementary schools nationwide, including Jefferson and several others in Texas. “There’s an openness and willingness to rethink these sites,” Turnbaugh said.
Related: Young children have unique needs and providing the right care can be a challenge. Our free early childhood education newsletter tracks the issues.
Nationally, districts of all sizes have embraced the trend over the past few years, including the Troy School District in Michigan and New York City Public Schools. In some cases, building a specialized facility helps a district with limited resources get “the biggest bang for their buck,” while meeting enrollment needs, said Turnbaugh. Some states and cities are also dedicating money to the efforts, including Illinois, Detroit and San Mateo, California.
That embrace is in part because of a growing recognition nationwide of the importance of play for young children, as well as reports that play time has been increasingly squeezed out of the early grades. States are also seeing record high enrollment in state-funded preschool programs. During the 2022-23 school year, investment in state-funded preschool reached an all-time high. Spending on the programs increased in 29 states, buoyed in part by Covid relief funds. Between 2022 and 2023, for example, Texas saw more than 21,000 additional 3- and 4-year-olds enroll. The state also slightly increased pre-K funding and, beginning in 2019, started requiring districts to offer full-day pre-K programs. The full-day programs have been rolling out in districts since 2020.
Scores of districts are “adding this new grade of 4-year-olds,” said Shelly Masur, vice president of advisory and state policy for the Low Income Investment Fund, which runs an initiative focused on creating and improving high-quality facilities for early learning programs. “They have to figure out where those kids are going to go.”
A facility built for their needs, like Jefferson, is exactly where young children should go, some experts say. The children seem to agree.
On a sunny fall morning, joyful screams could be heard as children chased each other up and down gentle hills on a large playground with natural-looking features meant to replicate the highlands and lowlands of Texas. Pre-K students in elementary schools don’t always have age-appropriate playgrounds, and structures are often designed for children who are older. But Jefferson has multiple large playgrounds and play courtyards, all designed for pre kindergarteners, featuring natural structures and textures, like logs and grass.
A playground at Jefferson Early Learning Center. Credit: Jackie Mader/ The Hechinger Report
In Alief, where more than 83 percent of children qualify as economically disadvantaged, more than 20 percentage points higher than the state average, residents voted in 2015 to approve a property tax increase to help pay for full-day pre-K programs in the district. After touring the Mansfield Independent School District’s early learning facility, Alief’s district leaders decided they wanted to invest in an early learning building with immersive, themed classrooms, instead of simply adding on or repurposing classrooms in elementary schools around the district. Jefferson opened in 2022 as one of two new early learning facilities in the district. About 6 miles away, the second, Maria Del Carmen Martinez Early Learning Center, which has a similar design, serves around 400 students.
A growing body of research shows that not all pre-K classrooms, or the facilities they’re housed in, are appropriate for young kids. Early learning settings in particular should have a warm, homelike environment with ample natural light, research shows. There should be spacious classrooms that allow children to move their bodies and play in a variety of spaces around the room. Facilities should have playgrounds that are appropriate for the littlest learners, and provide ample opportunities to experience and explore nature.
There are also practical details to keep in mind for preschoolers, like having bathrooms adjacent to classrooms, child-sized furniture, tiny toilets, and sinks low to the ground so children can practice routines like hand washing independently. “When we make things more accessible to them, they start to learn the independence that we need them to develop over time,” said Masur. This type of setting isn’t always present in elementary schools, which are built to accommodate a much wider age range of children and are typically designed for instruction rather than play.
Facilities can have a surprisingly large impact on the experiences of teachers and young children. A study of a preschool program in West Hartford, Connecticut, for example, found the amount of children’s time spent interacting with an adult caregiver increased from 3 percent to 22 percent after the program moved from a crowded basement room to a larger classroom with bathrooms, sinks, storage space and phones inside the classroom. Although all other factors remained the same, the teachers reported their students had fewer tantrums, something they attributed to having a larger, brighter and more organized space.
A facility can even affect how satisfied early educators are with their jobs. Delamore, the Jefferson teacher, who has worked in the district for 18 years, said the bright, spacious rooms and hallways help keep her from feeling “confined” during the day. While aimed at 4-year-olds, the building’s “calming atmosphere” helps her enjoy being at work, she said.
A student builds with blocks in a classroom at Jefferson Early Learning Center. The facility was built with 4- and 5-year-olds in mind and unlike elementary schools, revolves mostly around play.
Certain aspects make more sense for children at this age, she added, like the spiral shape of the building, which makes it easier to keep students together as they transition. Students eat family-style meals around circular tables, creating a sense of community, Delamore said, a contrast to the long, rectangular tables often seen in elementary school cafeterias.
Buildings that are not designed to meet childrens’ needs, or that are cramped and outdated, can impede development and learning, experts say.
One of the most recent examples of this comes from a 2016 study of Tennessee’s public preschool classrooms, which are mostly housed in existing elementary schools. That study, conducted by researchers at Vanderbilt University, found 25 percent of each school day was lost transitioning children to another activity, including walking to bathrooms and lining up to go to lunch.
When designing Jefferson, Turnbaugh and her team tried to “think of the campus through the eyes of a 4-year-old.” Delamore, at Jefferson, said the intricately-designed classrooms motivate students to go deeper in their play. On a recent morning in the “veterinary” classroom, a dozen 4- and 5-year-olds busied themselves around the room, immersed in play or small group work with a teacher. Children drew pictures of animals, read books and played animal-themed card games beneath large, colorful pictures of dogs and cats painted on the walls.
On one side of the room, 4-year-old Jaycyon had donned a white lab coat and was inspecting a fluffy gray and white toy cat lying on the counter in front of him. The cat was hurt, Jaycyon announced, likely from a sharp corner of the cage he was kept in.
“I have to give him a shot,” he said bravely. Jaycyon dipped a clear, plastic syringe into an orange medication bottle and confidently injected invisible medication into the cat.
At the end of three weeks, Jaycyon and his classmates will transition to a new classroom, such as “Tinker Town,” where they will learn about construction, or “Space City,” an homage to the nearby NASA space center.
On a daily basis, students have access to one of several outdoor spaces called a “back porch,” where families can also come and eat lunch together. These spaces also act as surrogate back yards for students, many of whom don’t have yards at home or access to parks. Students also have access to a sensory room with toys and soft mats, where they can take a break when they are overstimulated and practice skills to calm down.
Jefferson sits on nearly 20 acres of land, accessible via trails for students to explore with their teachers. (Alief returned the surrounding land back to its natural prairie state to help with climate-change related flooding.)
The educators at Alief say the district’s investment in a facility that encourages play-based learning has paid off. “What I see as a major difference is the children’s self-regulation, but also their confidence,” said the school’s principal, Kim Hammer, now in her 16th year leading an early childhood center. “A traditional pre-K setting is more teacher led and teacher directed,” she said. “Here it’s more teacher facilitated, so you see more of the children taking more initiative,” she added. “Children have autonomy, and children have much more choice.”
Two students play in a veterinary-themed classroom at Jefferson Early Learning Center. Each classroom is designed with a specific theme to encourage deeper play. Credit: Jackie Mader/ The Hechinger Report
There is evidence that the new facility may be helping children progress. During the 2023-24 school year, 49 percent of students came in meeting vocabulary benchmarks. By the end of the year, 73 percent were at that level, Hammer said, a higher rate than previous years when the district’s pre-K programs were in traditional elementary schools. School officials say the themed classrooms help enhance children’s language skills, as children learn the vocabulary specific to that room. Attendance rates are high and holding steady, something that is uncommon in pre-K.
Despite the success and benefits of programs like Jefferson’s, educators agree there are challenges. A pre-K only facility adds an extra transition for students who, in traditional programs, might otherwise attend pre-K at their home elementary school.
Without more funding, revamped pre-K facilities are unlikely to spread fast. Many districts lack the money, partly because state and federal funding for pre-K is often less than for other grades. In Texas, for example, although the state now requires districts to offer full day pre-K, it only provides funding for half a day of pre-K. Alief has to cover the rest from local funds.
Although sustaining the building will be financially challenging in the long run, educators are determined to find a way to make it work for the benefit of the kids.
Back at the veterinary center on that fall morning, Jaycyon finally had a breakthrough. He had discovered something alarming about his patient, or “kitty,” as he had been named by the pre-kindergarteners, that would direct his next veterinary tactics.
The Hechinger Report provides in-depth, fact-based, unbiased reporting on education that is free to all readers. But that doesn’t mean it’s free to produce. Our work keeps educators and the public informed about pressing issues at schools and on campuses throughout the country. We tell the whole story, even when the details are inconvenient. Help us keep doing that.
While consequential for all of higher education, pending and potential moves by the Trump administration that implicate funding could especially affect what has become an increasingly dominant aspect of multiple universities in terms of budgets and focus—academic medical centers (AMCs). AMCs are major funding recipients from the National Institutes of Health, the National Science Foundation and other federal agencies. AMCs and their health enterprises also are deeply connected to patient care programs like Medicare and Medicaid.
Media outlets covered the “confusion and chaos” that beset university presidents, medical center vice presidents, deans and researchers after the initial federal funding freeze. Now that the freeze has been temporarily rescinded, leaders of academic medical centers should move beyond confusion and chaos to focus on public presentations that emphasize their competence, compliance and cooperation with federal reviews. Now is an opportune time to pick up on President Trump’s recent emphasis on “merit” as the key to gaining federal support. University academic medical centers are well positioned to demonstrate and document their case.
To showcase “merit,” for example, a university academic medical center could cite ratings and commentaries about its successful NIH grant proposals, illustrating the talent and competitive advantages of its principal investigators and research teams. And they should emphasize that the NIH-funded research projects are not isolated: They are inseparable from a cooperative network within university health centers and hospitals. Evaluating these complex applied research alliances helps answer external questions about efficiency, effectiveness and significance of projects. The same kinds of questions are continually monitored in analysis of existing and new university degree programs for the education of medical doctors, nurses, physician assistants, pharmacists, medical technicians and health-care administrators. In addition to evaluating the training and preparation of researchers and health-care practitioners, an AMC pays systematic attention to accountability and responsibility for patient care and treatment as part of its daily and annual operations. These stories need to be told.
There are other sources that can be used to document AMC merit and performance. One can look at accreditation reports, specialized degree program reviews and financial balance sheets for the mosaic of health services and programs that are housed under the umbrella of an academic medical center. Institutional data can show that an academic medical center that aligns colleges of medicine and health care with such disciplines as biochemistry, physiology, bioengineering and statistics has evolved into a dynamic institution in which practice and advanced research are intertwined with providing professional services within a community.
A few summary statistics indicate this presence. The top 20 university AMCs each brought in more than $400 million in NIH research grants in fiscal year 2023. Within this group, Johns Hopkins University is first, with $843 million, followed by the University of California, San Francisco, with $789 million, and in third place, the University of Pennsylvania with $703 million. These are the peak of a cluster of 220 university medical centers in which academic programs such as the college of medicine partner with university medical foundations.
The fusion represents a new academic model in which the medical and health programs typically constitute about 60 percent or more of the total university budget. At universities with this structure, the AMC typically is home to a majority of the university faculty positions and student enrollments. The AMC also becomes a major economic force and employer in metropolitan areas and regional communities.
The academic health and medical complexes are economic engines. They often are the largest employer in the metropolitan area or even in the state, such as is the case for the University of Alabama at Birmingham and its health system. Universities in this category are the major provider of health services to large constituencies of patients. This academic health organization includes partnerships with Medicare, Medicaid and private insurance companies. Federal grants for research and service to the university often stimulate state financial support in terms of program grants and capital funding from state legislatures and governors and major gifts from foundations and private donors.
The message for “merit” is that these universities represent a new type of American organization—what might be termed the academic health business model. An abundance of quantitative and qualitative data makes external evaluation and detailed analysis of accountability possible. Sound policy evaluation from several constituencies—the executive branch, Congress, federal and state agencies, university leaders, and patient advocacy groups—calls for thoughtful, informed analysis to review and perhaps renew what has evolved as a distinctive academic enterprise.
A lively dialogue about the promises and benefits of AMCs that includes consideration of recent executive actions and potential future decisions, such as funding levels for Medicaid, is timely. The events of the last two weeks provide a much-needed moment for academic constituencies to reflect on what the expansion of AMCs means for individual research universities and higher education broadly in the future. If a funding freeze causes a chill for AMCs and their health enterprises, does the rest of the campus catch a cold, or even worse?
Recent presidential actions from Washington, D.C., have highlighted how much the budgets and identities of some research universities are more and more defined by their AMCs. In addition to helping AMCs continue to sustain and enhance their vital missions, all higher education groups need to contemplate the implications for universities whose mission and purposes are increasingly characterized and shaped by their academic medical centers.
John R. Thelin is University Research Professor Emeritus at the University of Kentucky. He is the author of several books on the history of higher education.
Neal H. Hutchens is a professor in the Department of Educational Policy Studies and Evaluation at the University of Kentucky. His research focuses on the intersection of higher education law, policy and practice.












{kind=link}